The major histocompatibility complex (MHC) is a group of genes that encode a variety of proteins important for immune function. These include cell surface markers and antigen-presenting molecules, which are responsible for recognizing “self” from “non-self” molecules to trigger immune responses against foreign pathogens. The MHC for humans is specifically termed the human leukocyte antigen complex, more commonly known as HLA. According to a genetics research article, the complex contains more than 200 genes, which code for different parts of these molecules through a variety of combinations of gene products. Therefore, there is a low chance of two individuals expressing identical HLA molecules. This is of great clinical significance as incompatible MHC molecules are a significant cause of transplant rejection.
Therefore, matching of donor and recipient antigens greatly increases the chance of graph acceptance in organ and tissue transplantation. However, there are few key differences in HLA matching requirements between bone marrow transplants and solid organ transplants. Bone marrow transplants, which are primarily used for blood diseases and immunodeficiencies, ideally occur between an HLA identical sibling recipient and donor. However, according to the National Marrow Donor Program, the minimal acceptable level of matching remains a 5 of 6 match for HLA-A, -B, and -DRB1 among HLA mismatched relatives and unrelated donors. On the other hand, the stringency of HLA matching requirements for solid organ transplants is much lower than for bone marrow transplants.
Image of the MHC from Brittanica
For bone marrow transplants, 10/10 matches indicate perfect compatibility across the key HLA loci between donors and recipients. According to recent research, These occur at HLA-A, -B, -C for Class I antigens and DRB1 and DQB1 for class II antigens. These matches typically occur from siblings or an unrelated donor from a matching registry. Such matches typically have a higher likelihood of success. When 10/10 matches are unavailable, haploidentical transplants are an alternative. These occur from a half-matched donor, which is typically between parents and their children or between siblings. This is because you receive half of your HLA from each biological parent. With mismatches at some of the key loci, haploidentical blood marrow transplants increase the likelihood of graft rejection
According to the Leukemia and Lymphoma Society, HLA mismatching greatly increases the risk of graft-versus-host disease (GVHD). his occurs when donor stem cells attack healthy stem cells. However, “the more HLA markers the donor and patient share, the greater the chance that the new immune system established by the donor cells will not attack the patient’s healthy cells.” Even if an unrelated donor is a perfect match, some patients may still be at risk for GVHD. There are many other risk-factors for acute GVHD, which typically develops within 100 days of transplantation. These include the older age of a donor or recipient and female donors for male recipients and vice versa. Therefore, a 10/10 match is preferred, paying close attention to these risk factors, in order to maximize the chance of bone marrow transplantation success.
Fire in the Gut: How Bacterial Imbalance Ignites Inflammation and Disease
This week, as we continue our discussion about the microbiome, we will get into the nitty gritty of how dysbiosis causes inflammation and subsequent autoimmune diseases. So, as a refresher, what is dysbiosis? This is the imbalance and/or lack of diversity between the beneficial and potentially harmful microbes within the human gut. One recent scientific study identified that elevated levels of LPS, an important cell wall component of some bacteria, may overactivate TLRs in gut epithelial cells, leading to increased production of inflammatory cytokines. TLRs, or toll-like receptors are a type of pattern recognition receptor (PRR) that allow the body to recognize foreign microbes and tissue damage. This dysbiosis-induced release of inflammatory cytokines, such as TNF, IL-1, and IL-6, leads to a colonic inflammatory response.
The same study found that pro-inflammatory cytokines disrupt intestinal tight junction proteins, disrupting the integrity of the intestinal lining. This causes leaky gut, which further increases inflammation by multiple pathways. Translocation through the gut barrier and into systemic circulation can allow bacteria to migrate towards the brain and other organs, triggering the production of proinflammatory cytokines in other parts of the body. Unlike the LPS themselves, cytokines can penetrate other barriers, such as the blood brain barrier, triggering further inflammation in the brain.
So, how do these pro-inflammatory cytokines impact the gut-brain axis? As a quick reminder, the GBA links the brain with gastrointestinal functions and the gut microbiome through neural and hormonal signals. Studies have found that pro-inflammatory cytokines also have an effect on the tight junction proteins of the blood-brain barrier. Subsequently, these also disrupt CNS localization pathways. In fact, the composition of the gut microbiota and related cytokine pathways have been found to affect different neurological disorders.
According to another study, breaches in the blood brain barrier can significantly alter the immune response to pathogens, leaving the central nervous system especially vulnerable to disease. More specifically, studies have found inflammation to have local effects on enteric neurons that stimulates CNS immune responses via the vagus nerve. Furthermore, proinflammatory cytokines and oxidative stress have been associated with neuron death. Therefore neuroinflammation, caused by proinflammatory cytokines that originate but in the gut and along the gut-brain axis have been linked to both neurodegenerative as well as intestinal diseases.
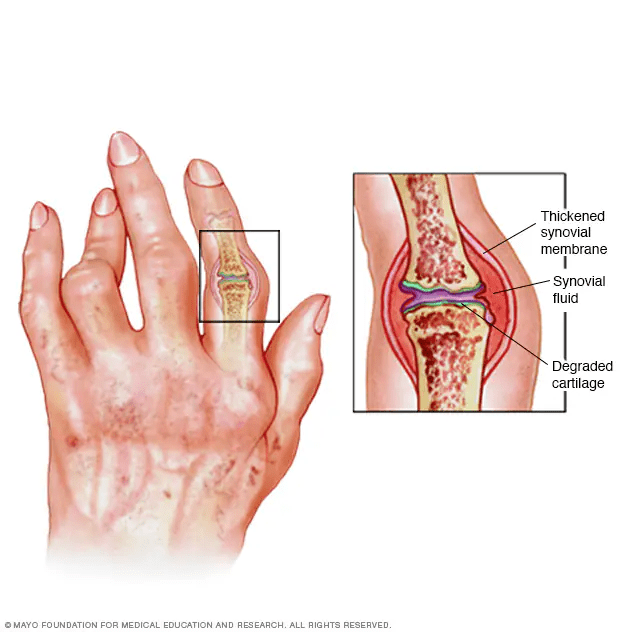
Image from Mayo Clinic
In addition to the disruption of the gut-brain axs, dysbiosis and pro-inflammatory cytokines have also been linked to a variety of autoimmune diseases such as rheumatoid arthritis. One of the most common autoimmune diseases, rheumatoid arthritis (RA) presents with progressive joint pain and inflammation. The cause is not completely understood, but is currently known as a complex interaction between genetic and environmental factors that suppresses the immune system. Before signs of inflammation, autoantibodies directed against their own cellular structures, like rheumatoid factor and anticitrullinated protein antibodies, are present in the blood, triggering autoimmunity across many parts of the body.
Among one study, an overabundance of the bacteria Prevotella. copri as well as the proliferation of the genus Collinsela and some Lactobacillus has been associated with the development of RA. These were associated with proinflammatory Th17 cytokine responses. Another study more generally noted that autoantibody production causes increased levels of proinflammatory cytokines in the joint synovium of RA patients. This occurs as growth factors and interleukins support Th17 differentiation and suppress the differentiation of regulatory cells, causing inflammation. Although this is a lot of immune system jargon and acronyms, it is important to note that changes in the microbiota are also linked to a host of other diseases through cytokine-induced inflammation, including multiple sclerosis and inflammatory bowel disease!
So we’ve all heard of the pesky seasonal flu, and most of us have likely contracted it at some point in our lives. This week, I want to explore this virus and its potential for an upcoming pandemic. The flu is an acute respiratory infection caused by the influenza virus. Seasonal epidemics typically occur during the winter months, characterized by fever, a dry cough, headache, muscle and joint pain, a sore throat, and a runny nose. Most recover within a week, however this virus can be severe among high-risk groups, resulting in hospitalization and even death. Human flu strains are primarily spread from person to person when infected individuals cough, sneeze, and talk.
Avian influenza, more commonly known as the bird flu, is an Influenza A that normally spreads between birds and other animals. Avian strains have adapted to better replication at higher temperatures of approximately 40°C, which is the typical body temperature for birds. However, sometimes humans can become infected with this virus. Although it rarely spreads from person to person, those who work with poultry, waterfowl, and livestock are most at risk. It is contracted if humans come in contact with an infected animal’s saliva, respiratory droplets, or feces.
The 1918 flu, also known as the Spanish flu, was the deadliest flu pandemic in the world to date. This microscopic killer was caused by a form of influenza A virus, and is thought to have begun as an avian influenza. The H1N1 strain developed mutations that allowed human mutation such as changes in proteins that improved binding to respiratory receptors. Contrary to its nickname, the first cases are thought to have occurred in the US, likely in military camps. This pandemic occurred in 3 waves, circling the globe from 1918 to 1919, near the end of World War I. Approximately a third of the world was infected, killing 50 million people worldwide. In fact, the United States alone lost 675,000 people to the pandemic, which is more casualties than both World Wars, the Korean War, and the Vietnam War Combined.
But why was this pandemic so much deadlier than other flu outbreaks? War-time conditions are thought to have contributed to the high death tolls including crowded living conditions, censored government information, and limited healthcare options. Also, antivirals weren’t around yet. Interestingly, younger adults in their 20s and 30s had a higher death rate. This is said to be because they hadn’t been exposed to that version of the flu before. Other theories state that their immune system may have overreacted, producing a cytokine storm that damaged healthy tissues. Death tolls were also high among military camps, with many flu infections followed by a secondary bacterial infection.
This post is especially relevant as the USDA, CDC, and FDA have recently expressed concerns regarding a current outbreak of the avian flu in US dairy cows, poultry, and now people in multiple states. The first confirmed case in dairy cows was March 25, 2024, and the first human infection was confirmed a week later. According to the USDA, there have been 169 new confirmed cases of the avian flu in cattle across three different states within the last 30 days. It has been confirmed that pasteurization is effective in inactivating the virus in raw milk. However, unpasteurized, raw milk is considered a high-risk food in terms of the avian flu as it may contain the live virus and serve as a transmission route to humans.
Unfortunately, the seasonal flu vaccine doesn’t protect against H5N1 bird flu. However, it is important to receive the vaccine to help prevent the risk of coinfection with the human flu and avian. Such dual infections, although rare, may allow genetic reassortment between the two strains, leading to new flu viruses that could pose a significant public health concern. Pigs may also be considered a vessel for genetic recombination as they can be infected with both avian and human strains. This is especially dangerous, similar to the 1918 pandemic, as such variants may be better adapted to infect mammals and humans. To try to stop the spread of this new avian flu, the USDA is offering the Dairy Herd Status Program with weekly herd testing to monitor the health status of dairy cattle. To encourage dairy producers to participate, the USDA is also offering financial assistance to enhance biosecurity and offset costs and losses associated with cattle flu tests, personal protective equipment and milk losses. Additionally, milk pasteurization standards have been emphasized. Lastly, surveillance systems have been implemented with genetic sequencing to track viral changes.
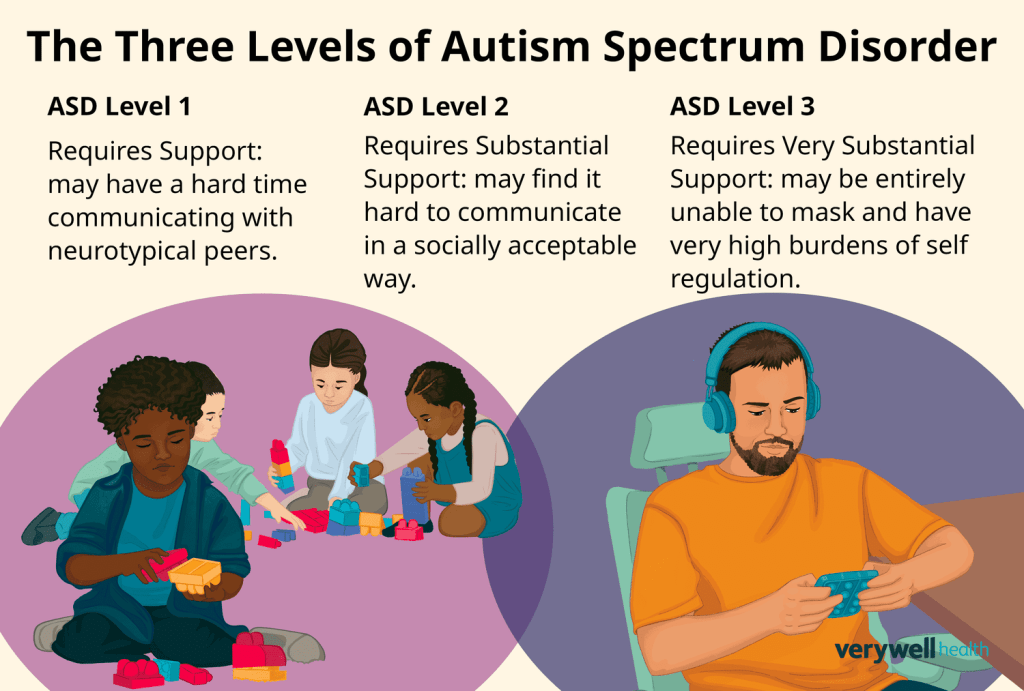
After our discussion last week on the false Wakefield claims, it feels only right to further investigate the actual underlying causes of Autism Spectrum Disorder (ASD) and its association with the gut microbiome. According to the CDC, ASD is a neurodevelopmental disability caused by varying differences in the brain, impacting the way individuals behave, communicate, interact, and learn. Symptoms typically begin before the age of 3 and are life-long. However, early intervention can significantly improve the development of a child with ASD. The presentation of ASD varies significantly from individual to individual as some have advanced conversation skills while others may be nonverbal. It is important to note that the DSM-5 now combines the separate conditions of autistic disorder, Asperger’s disorder, childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified into one “spectrum” ASD diagnosis.
Per the CDC, scientists currently believe there are multiple causes and risk factors for ASD that come together to shape development. According to scientific research, certain genetic conditions such as fragile X syndrome, tuberous sclerosis, down syndrome, and Rett syndrome put children at greater risk of ASD. Parents who are older or experience complications at birth are also more likely to have a child with ASD. Other pregnancy factors that have been found to play a role in the development of ASD, per the CDC SEED study, include fever during the second trimester of pregnancy, maternal autoimmune conditions, obesity, and diabetes, as well as prenatal exposure to air pollution and pesticides. Although neuropathological studies are limited, several studies have revealed subtle brain malformations including increased extra-axial fluid causing cortical overgrowth as well as problems with neuronal differentiation.
In recent years, scientific studies have begun investigating how the gut microbiome impacts the disease. According to one metanalysis, gut dysbiosis has been highly associated with ASD, although there is no distinct microbiota composition of those with ASD. Increased microflora and low microbial diversity is common of the ASD gut microbiota, which may contribute to the severity of autism symptoms by modulating the gut-brain axis. Specifically, an overgrowth of the genus Clostridium has been associated with ASD in multiple studies. Overall, the microbial imbalance known as dysbiosis is thought to increase the risk for ASD by altering the immune system and metabolism. Leaky gut syndrome, caused by dysbiosis, allows neurotoxic peptides and inflammatory cytokines to exit the gut, causing inflammation. This disrupts the neural, endocrine and metabolic mechanisms involved in gut-CNS signaling, which is involved with neuropsychiatric disorders such as ASD.
The connection between dysbiosis and ASD has also manifested through a wide range of GI abnormalities such as diarrhea, constipation, vomiting, feeding problems, acid reflux, and abdominal pain. In fact, according to one recent study, approximately 40% of those with ASD report gastrointestinal symptoms. It has been hypothesized that such complaints may worsen neurobehavioral symptoms by increasing anxiety, irritability, and social withdrawal compared to those without GI disturbances. Antibiotic treatment has been highly associated with long-lasting gut dysbiosis. Studies have found that the usage of antibiotics during the first 3 years of life alters the gut microbiome to significantly increase the risk of immunological and neurological defects.
The same metanalysis discusses microbiota transfer therapy as a promising new treatment to gut dysbiosis and ASD. This includes fecal microbiota transplantation (FMT), which works to transfer healthy bacteria from the feces of a healthy donor to the colon of an individual experiencing dysbiosis, according to John’s Hopkins. This is typically performed through a colonoscopy and is a common treatment for those with persistent Clostridium difficile infection. FMT rebalances the gut microbiome, and has been shown to improve behavioral symptoms in children with ASD. However, evidence is still insufficient to fully deem FMT as a practical and safe approach for ASD treatment.
According to multiple studies, this normalization of the microbiota through FMT may decrease intestinal permeability to reduce inflammation and improve immune function. FMT was also shown to improve GI symptoms in children with ASD. Sleep disturbances, which are common amongst those with ASD, were also shown to be reduced by FMT, demonstrating this as an effective treatment for sleep disorders as well. Higher quality sleep and GI function subsequently reduces other symptoms of ASD such as anxiety, irritation, and other extreme behaviors. Overall, interventions targeting the gut microbiome health are extremely important in both reducing risk for ASD and improving symptoms. Along with FMT, this may include dietary interventions as well as increased use of probiotics and avoidance of antibiotics.
With this winter’s flu season approaching, healthcare providers and public health officials are once again grappling with vaccine hesitancy among their patients, an issue that impacts not only individual health, but also collective wellbeing. This week, we will discuss the origins and progression of this hot topic, one ridden with misinformation and strong emotions.
In 1998, Dr. Andrew Wakefield and colleagues published a paper suggesting a link between the measles, mumps, and rubella (MMR) vaccine and the consequent development of autism. The infamous Wakefield Article specifically hypothesizes that the MMR vaccine caused intestinal inflammation that allowed proteins to enter the bloodstream and subsequently the brain. These proteins were suspected to cause a variety of developmental issues, including autism. The study supported such claims with a cohort of 12 children with developmental delay, 8 of which had autism. Each of these children had intestinal symptoms and developed autism within one month of receiving the MMR vaccine.
The Wakefield paper was retracted in 2004 as it was evidently based in scientific misconduct with fraudulent claims from misrepresented data. One of the many issues of this study design, as noted by Gerber in his literature review was that the self-referred cohort didn’t include unvaccinated control subjects. Therefore, it is impossible to determine a causal rather than coincidental relationship between the MMR and autism. In fact, about 90% of children in England receive the MMR vaccine between ages one and two, which corresponds to the age when autism typically presents and is diagnosed. Another major flaw with the paper was that authors claimed autism to be a consequence of intestinal inflammation. However, in reality the intestinal symptoms were observed after the symptoms of autism in all eight cases. Lastly, the participant assessments were not blind and the data was not collected systematically, causing the data to be riddled with bias.
Despite being retracted by the Lancet in 2010, Vaccine skepticism wildly increased following the publication of the Wakefield et al study. In fact, there was an immediate increase of 70 MMR injury claims per month. The public health impact has been widespread, with vaccine rates dropping in many countries. However, this fraudulent research has been disproven by numerous legitimate studies across multiple countries over the years. According to Gerber, by 2010, there were 20 studies of varying designs and locations that failed to support an association between the MMR vaccine and Autism.
One study linked hospital records to vaccination records of 537,303 children born in Denmark from 1991-1998. This large observational study by Madsen et al. included both vaccinated and unvaccinated subjects to strongly disprove the hypothesis of Wakefield. Finland researchers analyzed a cohort of MMR-vaccinated children from 1982-1996 and found 31 children with gastrointestinal symptoms and no vaccine-associated autism cases among 1.8 million children. This large prospective follow-up established that adverse outcomes of the MMR vaccine are extremely rare. Combined with the biological implausibility that the vaccine causes developmental delay, the statistical power of such studies with large cohorts have debunked the notion that vaccines cause autism. Therefore, the risks of measles, mumps, and rubella diseases themselves are much more dangerous than the vaccine.
Image from CDC article on addressing COVID-19 vaccine misinformation
In the wake of the COVID-19 pandemic, numerous false claims circulated the media raising fear of the newly developed vaccines. Conspiracy theorists claimed that the vaccines contained microchips for tracking and others raised unsupported concerns that the vaccine would cause infertility and pregnancy complications. Another widespread fear was that the COVID-19 vaccine could change human DNA. This claim gained traction through social media posts, anti-vaccine activists and celebrities, and even the misinterpretation of a 2021 published study that showed viral RNA can be reverse-transcribed and integrated into the genome of infected cells.
In response, experts explained that the mRNA vaccine “instructs the body to produce a protein found on the surface of the corona virus so that the immune system may learn to recognize and produce antibodies against this protein.” In disproving the claim, doctors and scientists note that the RNA doesn’t enter the nucleus at all and therefore doesn’t even come in contact with genetic material. Furthermore, research suggests that vaccine mRNA completely degrades within days. Large-scale clinical trials have also shown no evidence of genetic changes following COVID-19 vaccination, further supporting the biological and technical reasons why this is impossible. After all, for those of us vaguely familiar with biochemistry, we know that RNA and DNA have an entirely different chemical structure! This disproven claim, among the plethora of COVID-19 misinformation, emphasizes the importance of scientific literacy and public health communication
So far, we’ve discussed how lifestyle factors such as alcohol, fitness, sleep, and nutrition may contribute to gut dysbiosis. This week, we’ll expand on this to discuss how foodborne infections may contribute to this imbalanced state of harmful and beneficial bacteria in the gut. Also, we will get into a few bacterial-related public health topics including super bugs and super spreaders.
Diarrheal Infection and Dysbiosis
In fact, one study notes that blooms of Enterobacteriaceae, such as E. Coli and Salmonella, are some of the primary contributors to dysbiosis and subsequent inflammation. The immune response to these infections causes inflammation that damages the intestinal lining and promotes the overgrowth of harmful bacteria. This creates an environment that isn’t conducive to the normal microbiota, furthering dysbiosis. Furthermore, the overgrowth of infectious pathogens creates competition with beneficial bacteria for nutrients, furthering the imbalance. Other environmental alterations in the gut caused by infection include disrupted pH and altered oxygen levels, often favoring the growth of such harmful bacteria. More specifically, the same study noted that both Salmonella and E. Coli infections lead to the generation of nitrate in the inflamed intestine, which further supports their growth by anaerobic respiration. Another study on such infections, noted that the regulation of the gut microbiome through adequate nutrition and probiotics may aid in the prevention and treatment of diarrheal infections from Salmonella, Campylobacter, and E. Coli. Therefore, dysbiosis is both a cause and an effect of these infections.
So, what are the potential short- and long-term effects of bacterial diarrheal infections on digestive health? First off, most infections lead to inflammation of the gut and severe dehydration. According to the CDC, following salmonella infection, many people’s bowel habits don’t return to normal for a few months. Some may even develop reactive arthritis following infection, which is also the case with campylobacter cases according to the CDC. The long-term effects of E. Coli infection may also extend beyond digestive symptoms, as research has found those to be at increased risk for high blood pressure, renal problems, and heart disease later in life. According to the Cleveland Clinic, gas, bloating, poor digestion, abdominal pain, diarrhea, and constipation commonly occur immediately after infection as well as in the long term as symptoms of gut dysbiosis. Since these infections cause temporary or chronic inflammation and damage to the gut lining, the development of inflammatory bowel disease (ulcerative colitis, microscopic colitis, or Crohn’s disease) as well as inflammatory bowel syndrome (IBS) are also related to diarrheal infection and gut dysbiosis.
In recent decades, the overuse of antibiotics has contributed to antibiotic resistance and the development of “superbugs.” This is a growing global health concern, as antibiotics are virtually ineffective to treat certain pathogens, making it increasingly difficult to control their spread and prevent disability and death by such diseases. According to a research article on diarrhea-causing bacteria and their antibiotic resistance patterns, there have been many cases of antibiotic resistant Salmonella and Enterobacter. However, multi-drug resistance of E. Coli is one of the largest growing public health concerns in both “developing” and “developed” nations. According to the WHO, the misuse and overuse of antimicrobials in humans, animals, and plants is the primary cause of drug-resistant pathogens. This problem exists at countries in all regions and income levels, not only causing death and disability, but also leading to up to $1 trillion additional healthcare costs by 2050.
Factory Farming is a primary contributor to this growing global health concern. Antibiotics are commonly overused in low welfare factory farms to prevent the spread of disease among overcrowded animals. In fact, approximately three-quarters of all antibiotics sold each year are used in farm animals instead of humans. Bacteria on farms are consequently exposed to low doses of antibiotics, and those that survive reproduce rapidly. These bacteria then develop the ability to resist these drugs and others like them, passing resistance traits on to next generations. These antibiotics and related antibiotic-resistant bacteria then spread throughout the environment via manure through food, water, and soil contamination as well as through food supply chains when animals are slaughtered for meat. However, shifting farming practices towards better welfare methods and away from antibiotic use may help curb this rapid spread of antibiotic-resistant bacteria while promoting a more sustainable farm industry.
Mary Mallon, commonly referred to as “Typhoid Mary” was an Irish cook who worked in New York during the early 1900s. She became infamous as the first identified “typhoid super-spreader” in the United States. Multiple typhoid fever outbreaks were traced back to households where she was employed, and it was estimated that she infected up to 50 people throughout her career. Mallon was found to be an asymptomatic carrier of the disease, which was a relatively uncommon concept during this time. This caused health authorities to take drastic measures.
According to an article in the Smithsonian, when Mallon attested positive for typhoid bacteria in March of 1907, the Department of Health forced her into quarantine on North Brother Island just off the Bronx. She was released 3 years later, promising that she wouldn’t cook professionally again. However, she caused another outbreak 5 years later and was forced into quarantine again, where she lived the rest of her life. It is now known that up to 6% of those who recover for Typhoid fever remain contagious long after the active infection. Therefore, Mellon was certainly not the only known carrier for Typhoid at the time, raising bioethical questions of why she was the only one imprisoned for life. Some point to the notion that she was a relatively uncooperative Irish woman without a family, which led to discrimination. This case not only raised awareness for the dangers of asymptomatic carriers, but also brought up moral and public health issues regarding the deprivation of individual freedoms for a perceived greater-good.
This week, we will continue our discussion about the microbiome by exploring how different lifestyle factors influence the diversity and health of gut bacteria and therefore your overall health. We’ve all experienced that awful brain fogged feeling after a bad night of sleep. But, studies have actually shown that chronic reduced sleep quantity and quality may alter the composition of the gut microbiome– something that an afternoon nap may not fix. In fact this relationship is bidirectional as studies have also found that the microbiome composition may also influence sleep patterns. For example, higher levels of Faecalibacterium have been linked with longer sleep duration, while higher levels of Bacteroides have been associated with increased difficulty of falling asleep.
Overall, there is evidence that increased total sleep time is positively associated with total microbiome diversity. Disrupted sleep from conditions such as sleep apnea or insomnia has also been shown to alter the gut microbiome composition, decreasing the numbers of beneficial bacteria and increasing the harmful bacteria. More specifically, phyla richness of Bacteroidetes and Firmicutes has been associated with higher quality sleep. This strong association between sleep patterns and gut microbiome composition was also supported by studies that found a positive correlation between gut microbiome diversity and interleukin-6, a cytokine known for its effects on sleep. Ultimately, reducing hours of uninterrupted sleep harms the body’s natural circadian rhythm, which harms communication along the gut-brain axis, promoting an unhealthy gut microbiome.
However, sleep isn’t the only lifestyle factor shown to have intense effects on the gut microbiome! Regular physical exercise is another key player in promoting a healthy, diverse gut microbiome. According to one systematic review of evidence around this topic, women who perform at least 3 hours of exercise per week have increased A. muciniphila, a beneficial bacteria associated with lower BMI and increased metabolic health. Multiple studies have also associated higher cardiorespiratory fitness levels with a higher ratio of Firmicutes to Bacteroidetes. Increased levels of aerobic exercise and consequent maximal oxygen uptake (VO2max) has been shown to increase microbial diversity overall as well as the numbers of butyrate-producing species. Since butyrate feeds cells of the intestinal lining, this promotes a healthy gut barrier and prevents “leaky gut.”
Although there has been less research on the effects of strength training on the gut microbiome, this is also understood to have positive effects. According to another systematic review, no studies have found strength training to alter the composition or diversity of the gut microbiome, as was found with aerobic exercise. However, resistance training has been shown to reduce gut inflammation through multiple other mechanisms. One key biomarker of poor gut barrier function is zonulin, a protein that regulates the permeability of the intestine lining. Studies have reported significantly lower levels of zonulin amongst individuals who engage regularly in resistance training. Mucin biosynthesis has also been associated with resistance training. This is also important to preventing gut inflammation as mucin protects epithelial cells from stress-induced damage. By preventing leaky gut syndrome, resistance training consequently protects the gut microbiome.
With such profound effects on the microbiome, it is important to maintain quality sleep hygiene and regular physical exercise to promote a healthy and diverse gut microbiome. As we’ve discussed in previous posts, a healthy gut microbiome works wonders beyond improved GI functioning. In fact, the microbiome has extreme effects on the nervous system, endocrine system, metabolic system, and immune system pathways, as noted in this article posted by Stanford Lifestyle Medicine. The microbiome both regulates and produces neurotransmitters and hormones that are critical in mood regulation and overall mental-wellbeing. Improved sleep and exercise also promotes immune function and decreased inflammation by improving the diversity of the microbiome.
As we’ve suggested, improved quality sleep hygiene and regular physical exercise are an important treatment for gut dysbiosis. Many metabolic diseases such as obesity and diabetes have been associated with such gut microbiome dysbiosis through a variety of mechanisms in ample scientific studies. The gut microbiota is crucial in maintaining systemic homeostasis and overall wellbeing through the metabolism of nutrients as well as the maintenance of the immune system. Therefore, we should do our best to protect it with adequate levels of aerobic and strength exercise as well as improving our sleep habits. So, hopefully next time you will reconsider that afternoon coffee and decide to take your dog on a walk instead!
Hi guys, welcome back to the blog! Last week we discussed the impacts of ultra-processed food on the human microbiome. This week, I am excited to discuss another equally relevant hot topic: alcohol consumption. By the end of this week, I hope to have painted a picture of the importance of what we put in our bodies, both in the short and long term.
According to the Pew Research Center, 62% of US adults drink alcohol, and this consumption is on the rise. As we all know, binge drinking is especially common amongst college students, making this topic especially relevant for us. So, how does chronic alcohol consumption affect the composition of the gut microbiome? According to a scientific article published in Frontiers in Microbiology, there are several mechanisms through which alcohol causes gut dysbiosis: the neural pathway, the immune pathway, the neuroendocrine pathway, the metabolic pathway, and the inflammatory pathway. This begins when alcohol and its metabolites either inhibit or promote the growth of bacteria in the gut by causing inflammation and altering the acidity of the intestinal microenvironment. This typically doesn’t decrease the number of microbes in the gut, but instead alters their relative composition.
For example, according to the same Frontiers in Microbiology study, alcohol has been shown to increase the abundance of Proteobacteria, Enterobactericaea, Fusobacteria, which are gram-negative bacteria that increase LPS-induced inflammation. On the other hand, alcohol has also been shown to reduce the number of Firmicutes and Bacteroidetes which are major components of beneficial bacteria in the gut. Alcohol metabolism also promotes inflammation through the production of reactive oxygen species (ROS). Alcohol also directly damages the intestinal mucosa and leads to an overgrowth of bacteria that further contribute to this intestinal damage. According to a medically reviewed article posted by the MD Anderson Cancer Center, this contributes to “leaky gut syndrome,” as discussed in previous posts.
Not only do alcohol-induced changes in the microbiome cause inflammation and intestinal lining damage, but this dysbiosis has also been associated with addiction and associated behaviors and cravings. According to a research article posted in the International Journal of Molecular Sciences, studies have shown that alcohol addiction is associated with peripheral inflammation, such as leaky gut, caused by bacterial dysbiosis. This may be due to the immune response to chronic inflammation, which produces cytokines. When these continuously reach the brain, cytokines reduce the production of serotonin. This hormone-imbalance may eventually cause mood disorders including depression and addiction.
Also, according to an article posted on Nature, certain types of bacteria in the gut produce hormones and other molecules crucial to the brain’s functioning. For example, Bacillus makes dopamine, while Enterococcus produces serotonin. When the relative composition of these crucial microbes is altered by alcohol consumption, as discussed above, the production of these hormones is also altered. One study on rodents also linked the gut microbiome composition to the number of dopamine 2 receptors. This correlation found that changes in Lachnospiraceae and Syntrophococcus content may make individuals more susceptible to addiction. More generally, the microbiome composition has been associated with traits including impulsivity and susceptibility to stress and anxiety, which ultimately increases addiction-related behaviors.
I don’t know about you guys, but all this research definitely has me wondering if there is anything I can do to reduce these negative effects of alcohol. Although the best way to protect your gut microbiome is to reduce or cut out alcohol consumption, studies have actually found that probiotics may help mitigate such negative effects and even reduce addiction symptoms. According to the Cleveland Clinic, probiotics are live, beneficial microbes in food and health products that contribute to bacterial populations already in the body. These may help restore the gut microbiome balance, reducing inflammation and allowing the rebuilding of the gut mucosa. According to another research article posted on Frontiers in Pharmacology, probiotics have also been recognized to have antidepressant and anti-anxiety effects. This may reduce one’s susceptibility to alcohol addiction or reduce symptoms.
Additionally, according to the same article, some probiotics have been shown to reduce alcohol cravings and consumption through improved microbiota-gut-liver-brain axis communication. Probiotics may help restore gut symbiosis, increasing short chain fatty acid levels in the intestines. These metabolites are crucial to the functioning of the gut-brain axis, as discussed in the week one blog post. Probiotics may also reduce alcohol consumption and symptoms of addiction by altering the composition of bacteria involved in the reuptake of dopamine. Ultimately, studies have found that the long-term supplementation of live Lactobacillus and Bifidobacterium enhances cognitive functions and may be an effective treatment for alcohol use disorder.
Hi guys, welcome back to the blog! Thanks for following along with me as we continue to unpack the links between nutrition, the microbiome, and overall human health and well-being. In this week’s post we will be discussing another hot topic: Ultra-processed food.
We are constantly encouraged by the media and health professionals to limit our consumption of processed foods. But, what are processed foods? And this new, classically American, category: ultra-processed foods? Harvard Health describes processed foods as those with added salt, sugar, oil, or other substances that alter the food from its natural state. Such foods typically only include two or three ingredients with examples including canned fruits and vegetables, canned fish, salted peanuts, and freshly made breads. Although it’s definitely best to stick to whole, unprocessed foods, it’s ultra-processed foods experts have warned us to be most concerned about. Making up nearly 58% of total calories consumed in the US, these mysterious, industrial formulations are an everyday component of most people’s diets.
Ultra-processed foods have many added ingredients including sugar, salt, oils, fat, and starch. According to Yale Medicine, these additives are either extracted from food or composed of hydrogenated fats and modified starches. Synthetic ingredients are also high on the ingredients list in most ultra processed foods, relying on flavor enhancers, artificial colors, and preservatives. These additives not only increase their shelf-life, but make ultra-processed foods much more crave-worthy. The more obvious examples of ultra-processed foods include packaged desserts, breakfast cereals, soda, and chips. However, many foods that aren’t necessarily considered a “treat” are also ultra-processed, and equally as detrimental to our health. These include instant soups, hot-dogs, pasta, chicken nuggets, and packaged bread.
Image from FoodPrint on Ultra-procesed food
The literature is outstanding regarding the adverse effects of ultra-processed foods on human health. However, for this post, I am going to focus on the link between ultra-processed foods, the gut microbiome, and irritable bowel syndrome, otherwise known as IBS. According to the MayoClinic, IBS is a common chronic gastroenterological disorder that causes cramping, bloating, gas, and diarrhea or constipation. The disease affects the stomach and intestines, but its exact cause remains unknown. IBS has been linked to early life stress and other neurological issues including damage to the nerves in the digestive system. Even more commonly though, it has been triggered by severe viral or bacterial infection in the GI tract (gastroenteritis), or even a minor surplus of bacteria in the intestines. According to a Healthline article, studies have found the microbiota of those with IBS to be very different from that of healthy individuals. Although the causal link requires further investigation, it is clear that even if an altered gut microbiome doesn’t directly cause IBS, it definitely contributes to further inflammation and GI disturbances that further perpetrate the disease.
Photo from ISAPP Science Blog
According to a research article posted in the Clinical Gastroenterology and Hepatology journal, the synthetic additives in ultra-processed foods may alter the composition and function of intestinal microbiota: “Hence, ultra-processed foods could alter the concentrations of bacterial metabolites (ie, short-chain fatty acids), thereby increasing mucosal inflammation, disturbing the mucus barrier and intestinal permeability, which, in turn, may promote IBS pathogenesis.” In plainer terms, the poor nutritional quality of ultra-processed foods with low amounts of fiber and high amounts of sugar and saturated fats also takes a toll on the GI tract, leading to diseases such as IBS. Lastly, food intolerances and allergies may play a role in this link between IBS, ultra-processed foods and the gut microbiome, according to Healthline.
And before I conclude this post, I want to acknowledge a few of the ultra-processed foods that I consume on the regular. I love a good frozen pizza, followed by a bowl of ice cream. Or, when I’m on the go, I love to pack a bag of chips or an energy bar to get me through the day. Ultra-processed foods are indulgent and convenient. This makes them a topic worth discussing, because they are definitely here to stay.
So, If you didn’t get anything else from this post, I hope you remember that ultra-processed foods contribute to a cocktail of hidden health problems beyond classic weight gain. Although I am not one to discourage a treat from time to time, it is important to understand the role of these foods and their fake ingredients on our long-term health and wellbeing!
How do sugars and artificial sweeteners poison the microbiome?
Artificial sweeteners are on the rise due to their low-calorie content and ability to sweeten foods and beverages without raising blood-sugar levels. However, these sugar substitutes such as aspartame, sucralose, and stevia have many adverse effects on the body. According to a scientific review by Francisco Javier Ruiz-Ojeda et al, artificial sweeteners have been shown to disrupt the diversity and composition of the gut microbiome. This alteration leads to inflammation, glucose intolerance, and reduced short-chain fatty acid production. Madeleine Haase also noted that artificial sweeteners may increase intestinal permeability, a condition known as “leaky gut.” This allows bacteria to cross the intestinal barrier, which further triggers inflammation and immune responses. Haase also highlighted that some artificial sweeteners may cause otherwise harmless bacteria in the gut to form masses and invade cells in the intestinal lining, causing disease.
So, is it best to stick to simple sugars, when it comes to microbiome health? Unfortunately, the high consumption of glucose, sucrose and fructose have also been linked to changes in the gut microbiome. Gastroenterologist Dr. Suhirdan Vivekanandarajah explained in his blog post that table sugar has been found to inhibit the production of Roc, which is a protein required for the colonization of Bacteroides thetaiotaomicron. This bacteria is essential as it aids the body in processing vegetables and other healthy foods. Also, with a sugary diet, some sugars end up in the gut microbiome, providing excess energy for bacteria to multiply. This unwarranted growth may imbalance the composition of the microbiome. Like artificial sweeteners, unrefined sugar, especially high-fructose corn syrup, also leads to inflammation and decreased ability to regulate blood sugar due to decreased diversity in the gut microbiome.
How does a high-sugar diet increase Alzheimer’s risk?
These effects of sugar on the microbiome have been directly linked to a number of diseases, one of which hits a little too close to home for me, personally. As defined by the Alzheimer’s Association, Alzheimer’s is a progressive type of dementia that decreases memory and cognition. With no cure, prevention of Alzheimer’s is key, especially for those of you who, like me, have a family history of the disease. One key preventative measure is nutrition to help maintain a healthy gut microbiome. Leaky gut syndrome, as I mentioned earlier, allows the release of microbes into the bloodstream. In her review on the role of diet and the gut microbiota in Alzheimer’s disease, Sithara Dissanayaka noted that in combination with blood-brain barrier leakage, this may trigger neuroinflammation that contributes to Alzheimer’s. In fact, the systemic inflammation caused by a high-sugar diet and altered gut microbiome is a hallmark of Alzheimer’s.
Studies including the one by Sithara Dissanayaka, have linked high-sugar intake, microbiome dysbiosis, and elevated levels of amyloid-β, a protein associated with Alzheimers. Specifically, an abundance of Lactobacillus, a beneficial type of bacteria in the gut, was associated with lower levels of amyloid-β. Dissanayaka also highlighted a disrupted gut-brain axis as another contributor to Alzheimer’s. As discussed in last week’s post, the microbiome plays a key role in this communication system between the brain and the digestive system. Therefore, sugar-induced changes to the gut microbiome composition can alter this communication, further contributing to Alzheimer’s.
Image by Sithara Dissanayaka, depicting the findings of her study on gut-brain-microbiome interactions
What does a sugary diet look like?
I don’t know about you, but this discussion of sugars and the microbiome will definitely have me rethinking my added sugar consumption! In doing so, it is helpful to have an understanding of how much sugar is actually in some of my favorites. The amount of sugar in foods is always listed on the nutrition label in grams. In order to conceptualize this, it’s helpful to understand that 4 grams of sugar is equivalent to 1 teaspoon. Some foods are obviously high in sugar, such as a small Chick-Fil-A vanilla milkshake with a whopping 21 teaspoons of sugar. However, there are many foods with equally shocking amounts of added sugar that you would never expect.
Image of a variety of yogurt brands from a blog on healthy yogurt choices
For example, Chobani Greek yogurt, which has always been a breakfast staple that I have considered healthy. The Chobani Flip Almond Coco Loco has a 18g of sugar, 14 of which are added sugars. The second ingredient is cane sugar and honey is not far down on the list. Yogurt is advertised as being a probiotic rich food that is great for gut health, however 4.5 teaspoons of sugar in a single portion surely counteracts these benefits.
The American Heart Association recommends that men should consume no more than 9 teaspoons of added sugar per day. For women, this recommendation is 6 teaspoons. The average American consumes an average 17 teaspoons of added sugar per day, far exceeding the recommendations. The majority of my sugar consumption comes from sugary beverages (I love a vanilla latte!), protein bars, and other sneaky forms of sugar such as yogurt and bread. As a pre-PA nutrition major, I would say that I prioritize healthy eating. To do so, I try to avoid eating out and limit processed foods in my grocery runs. However, this is often time consuming and expensive. Therefore it is unsurprising to me that the average American is consuming 2-3 times the recommendation of added sugar, truly a public health epidemic!